Sciatica
Sciatic nerve damage in an acetabular fractures — IJGM Dove Medical Press
Introduction
Acetabular fracture can be a devastating intra-articular injury that is more frequent in men. 1 These fractures are usually high-energy and can be sustained in road traffic collisions (RTAs) as well as falls from heights. 2,3 Most fractures of the acetabulum are caused by polytrauma that affects the thorax, brain abdomen, extremities or any other region. The traumatizing sciatic nerve injury is among the most serious injuries that can be associated with an acetabular fracture. 4,5
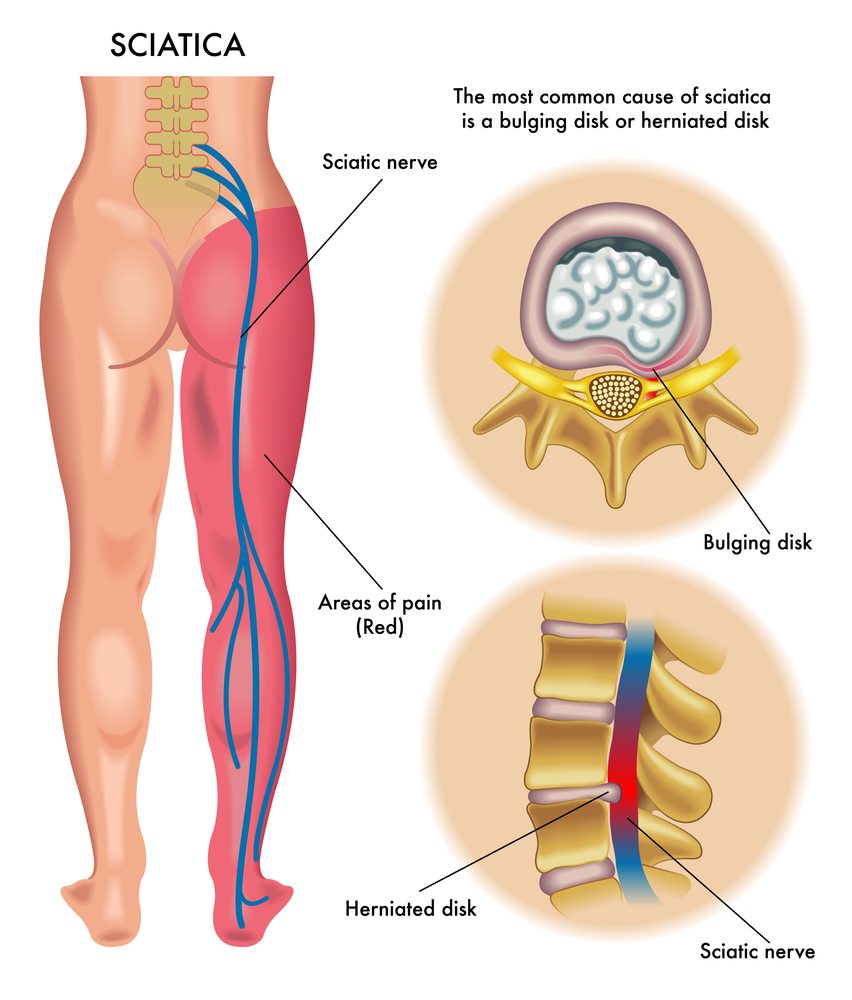
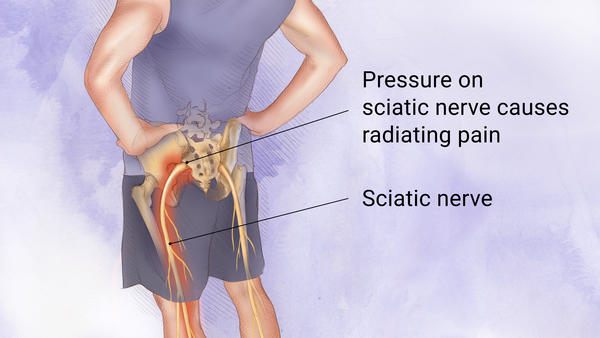
Sciatic nerve is the most extensive and longest nerve within the body. This is the main motor nerve that supplies the hamstrings, foot muscles, and calf muscles as well as a crucial sensory nerve that supplies the calf and foot. The motor and sensory functions of nearly all the areas beneath the knee are supplied through the sciatic nerve. 6,7 The common branch that is part of the sciatic nerve extends deep into the gluteus maximus. It is close to the acetabulum which is separated from hip joint with just a tiny amount of soft tissue. Thus, it is believed that the sciatic nerve is extremely vulnerable to injury because of a fracture that has been displaced or dislocated the femoral head. 8,9 Incorrect diagnosis and treatment can cause a serious effect on the functioning of the lower extremity affected.
Acetabular fractures that are accompanied by the traumatic the sciatic nerve damaged is grave accident with a reported frequency of 3.3-33 percent in all instances of Acetabular fractures. 4,10,11 Letournel and Judet 12 discovered that the highest frequency in sciatic nerve injury was in conjunction with an anterior fracture or dislocation in the joint of the hip. Issack as well as Helfet 13 found that all patients who suffered from post-traumatic sciatic nerve injury had the pattern of fracture that was present in the posterior wall and posterior column. There are however, little studies of the acetabular fracture in conjunction with trauma to the sciatic nerve injury. 4 Furthermore the majority of studies have pooled trauma and iatrogenic injuries to study or included sciatic nerve injury in conjunction with other nerve injuries to the hip. A few studies have focused exclusively on the traumatic sciatic nerve injury. 4,14
The study examined the characteristics of patients suffering from an acetabular fracture that is accompanied by traumatic sciatic nerve injury, as well as the characteristic clinical features of the patients, and tried to identify risk factors that could cause traumatized sciatic nerve injury that is associated with an acetabular fracture.
Materials and Methods
Our retrospective analysis identified patients with an acetabular fracture in our trauma center from January 2014 to June 2021. All patients were treated at Shandong Provincial Hospital. Shandong Provincial Hospital Affiliated to Shandong First Medical University. Study was approved by Medical Ethical Committee of the institute of the authors. This study is compliant with the Declaration of Helsinki. The patients who participated in the study gave their informed consent (the patients who were under 18 years old signed an informed consent form by the legal guardian or parent of the patient) and all data was anonymized prior to analysis to ensure privacy of the patient.
The data was gathered about sex, age as well as the mechanism of injury. Injury Severity Score (ISS) as well as the Abbreviated Injury Scale (AIS) score, as well as the associated fractures, types of fracture, based on the classification system of Letournel-Judet, fifteen whether or hip dislocation was present, and whether sciatic nerve injury was present, and different types that can be caused by sciatic nerve injury.
According to the Letournel Judet classification the acetabular fractures are identified by two attending orthopaedic surgeons in traumatology. If there is disagreement, a senior doctor will examine that the diagnosis is accurate. For data that contain subjective elements such as ISS or AIS score Two researchers must strictly adhere to the scoring guidelines to assure the accuracy of the scoring.
Statistics Analysis
The measured information (age, the ISS score, AIS score, etc.) are reported as the mean + standard deviation as well as count data (sex and mechanisms of injury, injuries, etc.). Normally distributed information and variables that impact the risk of the possibility of traumatic nerve injury were analyzed. nerve injury were assessed with Fisher’s exact test and the Chi-square test. The degree in Sciatic nerve injury was considered the independent variable. The variables that were found to have with a significant P-value of <0.05 for univariate analysis were incorporated into the Multivariate Logistic Regression Model. The statistical analysis was conducted with SPSS software version 24.0 (IBM Corp., Armonk, NY, USA). The P-value of <0.05 was considered to be statistically significant.
Results
General Information
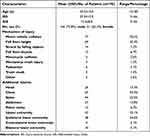
There were 195 subjects (144 males, 51 females) with complete radiographic and clinical data were eligible to participate for the research. The median of age ranged from 43.5 years (range 15-85). MVC (motor accident with a vehicle) occurred as the main frequently reported reason for injuries (in 39.5 percent of instances) and was followed by falls from a height (in 35.4 percent) (Table 1.).
|
Table 1. Demographics, Trauma Scoring Mechanism of Injury, and Additional Injuries |
The mean ISS score was 25.9 (range 5 – 66) and the median AIS score of 12.4 (range 3 to 56). The associated injury was observed in 72.3 percent of cases. The most frequent incident was a chest then lower extremity fractures, spinal injuries. Seven out of these 44 spinal injuries were related to those of the spinal cord (including one case of bilateral acetabular twists) (Table 1.).
Aftabular Fractures: Classification
9 of the 195 participants had an acetabular injury, resulting in an aggregate of the 204 fractures of the acetabulum. Posterior wall injuries were the most frequent type, followed by transverse fractures in the shape of a T as well as anterior and transverse wall wall fractures and anterior columns fractures. Lateral column fractures, wall and column fractures and anterior column hemi-transverse cracks, and anterior wall fractures are uncommon (Table 2.).
|
Table 2. of Fracture Classification, and the Related Injury Acetabular Fractures |
Seventy-one sides were paired with hip dislocations: 52 patients were posterior dislocations 19 suffered from central dislocations and none were anteriorly dislocated (Table 2.).
Twelve patients suffered head fractures in the femoral region. The fractures affected the wall’s posterior in four cases. They were T-shaped fractures in two instances, transverse fractures in two cases, as well as anterior and transverse wall fractures in two cases (Table 2.).
The types of sciatic Nerve Injuries
Inclusion of patients suffering from spinal cord trauma (7 cases eight sides) and Iatrogenic sciatic nerve injury (2 cases two sides) 18 (9.7 percent) out of the remaining 186 people suffering from Acetabular fractures suffered the traumatic sciatic nerve injury and it occurred bilaterally in one instance. Four (21.1 percent) from the 19 side that sustained traumatized sciatic nerve injury were afflicted by one common peroneal nerve division. The other 15 (78.9 percent) were affected by all the typical peroneal as well as the tibial nerve divisions. There were no instances of tibial nerve division injuries.
The Comparison of Patients Based on the Status of Traumatic Sciatic Nerve Injury
Baseline
There were significant differences between groups with respect to these variables: the ISS as well as the AIS score, as well as the frequency of acetabular injuries that were combined with abdominal trauma to the upper part of the body as well as bilateral lower extremity fractures and the rate of shock hemorrhagic. There was no distinction in sex, age the cause of injury or any other injuries or injuries that are combined in the groups (Table 3).).
|
Table 3. Demographics and the characteristics of injuries for patients suffering from as well as without Nerve Injury |
Comparative Analysis of the Type and frequency of hip dislocation and Femoral Head Head Fracture between the two groups
In the study group that did not suffer from sciatic nerve injury the posterior wall fractures were the most frequent type of acetabular break (20.6 percent 36/175) The next most common type was T-type fracture (19.4 percent) and fractures between the two columns (18.3 percent). For those with sciatic nerve injury the most prevalent kind of fracture affected both columns (26.3 percent 5/19) then T-type fractures , as well as the transverse and posterior wall fractures (15.8 percent (3/19). It was not evident that there is a significant differences in the probabilities of a specific type or type of fracture ( P>0.05) other than for fractures of the anterior column that is the acetabulum ( P<0.05) (Table 4).
|
Table 4 Fracture Pattern and Related Injuries for Patients With and without a Nerve Injury |
Posterior hip dislocations were observed in 9 of the sides (47.4 percent) for the patient suffering from sciatic nerve injury, and 38 (21.7 percentage) for the one with no sciatic nerve injury. The within-group distinction was significantly different ( P<0.05). The study did not show any significant differences in prevalence of hip dislocations at the central hip between groups with as well as without nerve injuries (2 sides [10.5 percent] vs. 16 sides [9.1 percent]; P>0.05) or in the relative frequency of fractures to the femoral head (2 [10.5 percentand 10 [5.7 percentin the group with sciatic nerve injury (2 [10.5%] vs 10 [5.) (Table 4, Table).
Risk Factors that Increase the Risk of Traumatic Sciatic Neuro Injury
To limit the impact of confounding factors on every variable that might be a factor variables that statistically significant in univariate analyses, such as those relating to ISS, AIS score, bilateral lower extremity fractures posterior column fracture, as well as hip dislocations that are posterior were analyzed in the multivariate logistic regression. A greater AIS score and posterior column fracture and the posterior dislocation of the hip joint were found as predictors of the acetabular fracture, which is accompanied by traumatized nerve injury. nerve injury (Table 5).).
|
Table 5 Multivariate Logistic Regression Analysis of Risk Factors for Traumatic Sciatic Neuron Injury |
Discussion
Acetabular fractures are a serious injury that is usually result of high-energy injuries including falls from heights, RTAs, as well as falls from heights. 16,17 With changes in the transportation and construction industry there have been some adjustments in the prevalence and the characteristics for acetabular injuries. Kelly et al 18 carried out an analysis meta-analysis (using data from 2005 to 2018) initially released in Giannoudis et al 19 in 2005 (using data from 1980-2003) to bring up-to-date information about patients with acetabular injuries as well as the mechanism of injuries, treatment of complications, as well as functional outcomes. Their findings revealed rising average patient’s age between 38.6 years 45.2 years. There was also a drop in the percentage of injuries caused by RTAs, from more than 80 percent to 66.5 percent as well as an increased number of falls-related injuries from 10 25 percent to over 10. Research conducted across the globe has also concluded that falls caused by RTAs and falls from height are the most common causes of acetabular fractures in which the bulk of fractures are suffered by males. 14 In the current study, the average patient’s aged 43.5 years. 73.8 percent were males and the injuries occurred in an MVC at 39.5 percent of the cases and because of an injury sustained from a fall at 35.4 percentage This is in line with reports from the literature.
Acetabular fractures can be connected to multiple injuries within other parts within the human body such as the chest, brain abdominal, extremities, and various other areas. Further fractures as well as chest head, abdominal, and head injuries are the most frequent. 18 However the ISS scores that have been published in the literature are varied and ranged between 21.4 + 11.9 during a research study done by Simske and colleagues up to 15.9 + 12.5 for a study done by Kelly et al 4,18 In addition, the mean score of the ISS in a review of patients at 29 medical facilities was 13. 8. Only 3 percent of the patients who participated in the study had polytrauma, and had an average score of 21 + 11. 9 In our study, the majority of patients sustained multiple injuries which included chest injury (32.8 percent) as well as lower extremity injuries (31.8 31.8 %)) among them) being most frequent. The median ISS along with AIS score was 25.9 + 10.4 as well as 12.4 + 8.0 respectively, which indicates serious injuries. The high scores could be due to the fact that the study was carried out at a single , level III trauma center (equivalent to an I-level Trauma center located in Western countries, such as in the United States and Germany) in which the majority patients suffer from multiple and serious injuries. Some are referred to our center for treatment of more complex injuries following stabilization in local hospitals.
Based on the Letournel-Judet classification method, the majority of frequent types of fractures involved the posterior wall or are associated with T-type and column fractures. Based on the reason for damage, the most prevalent kind of acetabular fracture that is that is associated with the MVC included a fracture of the posterior wall (27.3 percent 21/77) and then fracture in both columns (18.2 percent). Falls from high elevations were the most frequent source of T-type injuries (27.6 percent) and were followed by injuries to both columns (26.1 percent) along with posterior wall wall fractures (15.9 percent). The majority (64.6 percent) of fractures of the acetabulum that affect those in the posterior wall (posterior wall fractures, the posterior column, the transverse wall and the posterior wall) were caused by the posterior dislocation of hip. Acetabular fractures that are accompanied by head fractures of the femur are rare being seen in 6.2 percent of the patients studied in our study. These findings are in line with other reports. 4,9,20-22
The concomitant the sciatic nerve injury is among the most severe complications of an the acetabular injury. Uncorrect diagnosis and treatment could negatively affect the lower extremity’s performance. 11,13 In our study, the frequency of acetabular fractures that were accompanied by traumatized nerve injury was 9.8% (19/194). nerve injuries was 9.8 percent (19/194) of which 4 (21.1 percent) were involving in the peroneal common nerve division, and 15 (78.9 percent) were affected by equally the common peroneal as well as the tibial nerve divisions. There were no instances of tibial nerve division injuries in our study. In the study of Simske et al 4 the common peroneal nerve branch was damaged in 68.0 percent of instances (17/25) while the whole sciatic nerve was injured in 32.0 percent (8/25). Also, there were no cases with isolated the tibial nerve branch trauma. However, the results from many studies that have examined the acetabular injury and sciatic nerve injury are in line in our research findings. The peroneal nerve division is more likely to suffer injury as compared to those of the tibial nerve division. The primary causes are as the following: (1) lower excursion of the peroneal nerve due to the tethering of the nerve at the fibula’s neck as well as the larger sciatic notch (2) Peroneal nerve division is comprised of fewer nerve bundles that are smaller in size and are separated from connective tissues less than it is for the tibial division also (3) that the division peroneal lies along the lateral aspect of the sciatic nerve The fracture or femoral head gets displaces inward, backward and upwards and the peroneal root is compressed or pierced first. 11,13,14,23
In this study, we discovered that age, gender and the injury’s cause had no effect on the risk of acetabular injury and sciatic nerve injury. This corresponds to the results of previous research. 4,14 The rate of the traumatic nerve injury was significantly increased. nerve damage was significantly hindered by the presence of an upper abdominal organ injuries and acetabular fracture, which was accompanied by bilateral lower extremity fractures, the severity score of trauma as well as the rupture of the posterior column in the acetabulum and a posterior dislocation that is combined with the hip joint. We utilized the multivariate logistic regression method to determine the most statistically significant factors that predict the sciatic nerve injury. In univariate analyses the there was evidence that sciatic nerve injuries were more common in those suffering from an injury to the upper abdominal organs However, there was no correlation observed with multivariate logistic regression.
Most acetabular fractures occur as caused by high-energy force that is transmitted to Acetabulum by an lower extremity. fractures in the acetabulum when coupled with lower extremity fractures are not uncommon. The probability that a nerve injury to the sciatic nerve damage was substantially greater in cases where an acetabular injury was coupled by bilateral lower extremity injuries this could be due to the fact that patients suffering from two lower extremity fractures in a row are more likely to suffer more intense injuries to the acetabulum which can cause damage to the sciatic nerve. In addition, a logistic regression analysis failed to find any connection with Sciatic nerve damage and lower extremity fractures in bilateral that could be due to the low sample size, and also the results being somewhat asymmetrical.
The severity score for trauma can indicate the patient’s health and prognosis up to a certain degree, and the values of the ISS and AIS are often used to determine the severity of the injury. 24-27 Sciatic nerve injury is reported to be related to trauma severity scores for patients with acetabular injuries. 4,18 The more injuries a patient experiences more, the greater the risk of suffering a trauma-related and sciatic nerve injury. Simske et al 4 discovered that the median ISS score was substantially higher in patients suffering from nerve injury than with no nerve injury. In our study we found that the ISS value as well as the AIS score were significantly higher in patients that suffered from the traumatic sciatic nerve injury. Logistic regression analysis found how the AIS score was significantly associated with the injury.
Traumatic sciatic nerve injury is common among patients suffering from fractures of the posterior wall, or the posterior column in the acetabulum as well as the posterior dislocation of the hip joint. It is also linked to the cause of this kind of trauma. 4,28,29 Unlike previous research however, we observed that none of the types of fractures that involved the posterior column had an impact on the probability that the sciatic nerve injury, not even those that involved an anterior wall. When we looked at logistic regression it was evident that there was significant differences in the frequency that posterior column fractures occurred in groups that had and those with no the sciatic nerve injury. However, the smaller number of patients with only minor posterior column fractures might influence the results. There is evidence that hip dislocations in the posterior region are the primary reason for sciatic nerve injury in patients suffering from Acetabular injuries. 4,30 In our study, the risk of posterior dislocations of hip joints was more frequent in those that suffered from Sciatic nerve injury. The possible reason for this is that the damaged hip joint caused the gap between the sciatic nerve and the acetabulum or femoral headmore pronounced, which could increase the risk of nerve injury. The study revealed that hip posterior dislocation was the most significant risk reason in the sciatic nerve injuries in univariate as well as multivariate logistic regression analyses, which implies that Sciatic nerve injuries are more common with posterior dislocations in the joint of the hip. Dislocations of the hip in the central region and femoral head injuries did not have a significant effect on Sciatic nerve.
The study is not without its issues, including an retrospective design as well as a smaller sample size. But, these kinds of cases are not common, and larger multicenter studies may be expected in the future.
Conclusions
Acetabular fractures are typically high-energy and often coupled with other injuries. Posterior wall, double-column and T-type fractures are among the most commonly encountered types of fractures. Acetabular fractures with trauma that is severe have a higher chance to occur by Sciatic nerve injury. There is no connection with Sciatic nerve injury and sexual age, the cause of injury or fracture type central hip dislocation or head fractures of the femoral bone. The study showed that a single posterior wall fracture in the acetabulum didn’t significantly impact the risk for Sciatic nerve injury. Acetabular fracture, when combined with posterior hip joint dislocation was the most significant predictor of the sciatic nerve injury.
Abbreviations
ISS ISS, Injury Severity Score. Abbreviated Injury Scale, AIS; MVC, Motor vehicle collision; RTA, Road traffic accident.
Data Sharing Statement
All the data gathered or analysed during the study are contained in this paper. Any further questions can be directed to the author responsible for the study.
Ethics Approval, Informed Consent and Ethics Approval
The experimental protocol was developed in accordance with the ethical guidelines in the Helsinki Declaration and approved by the Human Ethics Committee of Shandong Provincial Hospital affiliated with Shandong First Medical University. A written informed consent form was received from all study participants.
Consent to Publication
Each author contributed significantly to the study published, whether it was in the design, conception of the study, design, implementation and acquisition of data the analysis or interpretation of data, or any of these areas. They participated in drafting, revising , or critically reviewing the paper; provided final approval for the version to be published. they have a consensus with the journal to which the article is submitted, and have agreed to take responsibility for all aspects that the article is based on.
Finance
The study was funded through Shandong Province Major Scientific and Technical Innovation Project (No. 2021SFGC0502 Shandong Province Major Scientific and Technical Innovation Project (No. 2021SFGC0502) and which is the Shandong Provincial Natural Science Foundation (No. ZR2020MH088; No. ZR2021MH013; No. ZR2021QH307) and Shandong Province Key research and development program (No.2017GSF18112). They, the authors’ immediate family members and any research foundations to which they are affiliated with have not received any financial and other benefits or compensations from any other commercial organization related to the subject matter of this article.
Disclosure
The authors are all free of conflicts of interest with respect to this article.
References
1. Laird A, Keating JF. Acetabular fractures: a 16 year prospective study of epidemiology. J Bone Joint Surg Br. 2005;87(7):969-973. doi:10.1302/0301-620X.87B7.16017
2. Mauffrey C, Hao J, Cuellar DO, et al. The epidemiology and the patterns of injury of acetabular injuries: are both the USA and China similar? Clin Orthop Relat Res. 2014;472(11):3332-3337. doi:10.1007/s11999-014-3462-8
3. Rinne PP, Laitinen MK, Huttunen T, et al. The frequency and the trauma-related mechanisms of acetabular injuries: a national study conducted in Finland between 1997 and 2014. Injury. 2017;48(10):2157-2161. doi:10.1016/j.injury.2017.08.003
4. Simske NM, Krebs JC, Heimke IM, et al. Injury to the nerve with Acetabulum fractures: prevalence and factors that influence the recovery. J Orthop Trauma. 2019;33(12):628-634. doi:10.1097/BOT.0000000000001604
5. Ahmed M, Abuodeh Y, Alhammoud A, et al. The epidemiology of acetabular fractures in Qatar. The Journal of Orthop. 2018;42(9):2211-2217. doi:10.1007/s00264-018-3824-z
6. Kanawati AJ, Narulla RS, Lorentzos P, et al. The shift in the direction that the sciatic nerve in the posterior approach towards the Hip. Bone Joint J. 2015;97-b(8):1056-1062. doi:10.1302/0301-620X.97B8.35746
7. Isin Y, Hapa O, Kara YS, et al. The study is a CT investigation of sciatic and femoral nerve periacetabular movement in various hip positions. J Orthop Surg Re. 2020;15(1):404. doi:10.1186/s13018-020-01937-7
8. Kline DG, Kim D, Midha R, et al. Treatment and outcomes from the sciatic nerve injury: A twenty-year experience. J Neurosurg. 1998;89(1):13-23. doi:10.3171/jns.1998.89.1.0013
9. Lehmann W, Hoffmann M, Fensky F, et al. What is the prevalence of nerve injuries that are associated with fractures of the acetabulum? Clin Orthop Relat Res. 2014;472(11):3395-3403. doi:10.1007/s11999-014-3838-9
10. Foulk DM, Mullis BH. Hip dislocations: Evaluation and treatment. J Am Acad Orthop Surg. 2010;18(4):199-209. doi:10.5435/00124635-201004000-00003
11. Fassler PR, Swiontkowski MF, Kilroy AW, et al. The sciatic nerve caused by acetabular fracture. J Bone Joint Surg Am. 1993;75(8):1157-1166. doi:10.2106/00004623-199308000-00005
12. Letournel E, Judet R. Fractures of the Acetabulum. Springer Science & Business Media (2012).
13. Issack PS, Helfet DL. Sciatic nerve injury that is associated with acetabular fractures. HSS Journal. 2009;5(1):12-18. doi:10.1007/s11420-008-9099-y
14. Stavrakakis IM, Kritsotakis EI, Giannoudis PV, et al. Sciatic nerve injuries after Acetabular fractures: A study of the incidence and consequences. Eur J Trauma Emerg Surg. 2022;48(4):2639-2654. doi:10.1007/s00068-022-01896-0
15. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification as well as surgical options to open reduction. A preliminary report. J Bone Joint Surg. 1965;46(8):1615-1646. doi:10.2106/00004623-196446080-00001
16. Melhem E, Riouallon G, Habboubi K, et al. The epidemiology of pelvic and Acetabular breaks in France. Orthop Traumatol Surg Res. 2020;106(5):831-839. doi:10.1016/j.otsr.2019.11.019
17. Lundin N, Huttunen TT, Berg HE, et al. The prevalence in acetabular as well as pelvic injuries. A study across the country of 87,308 injuries over the course of 16 years in Sweden. Injury. 2021;52(6):1410-1417. doi:10.1016/j.injury.2021.03.013
18. Kelly J, Ladurner A, Rickman M. Surgical treatment of acetabular fractures A review of the literature in the present. Injury. 2020;51(10):2267-2277. doi:10.1016/j.injury.2020.06.016
19. Giannoudis PV, Grotz MR, Papakostidis C, et al. Operative treatment of fractures that have been displaced of the Acetabulum. A meta-analysis. J Bone Joint Surg Br. 2005;87(1):2-9. doi:10.1302/0301-620X.87B1.15605
20. Magu NK, Gogna P, Singh A, et al. Long-term results following surgery to treat the acetabular posterior wall fractures. Orthop Traumatol Surg Res. 2014;15(3):173-179. doi:10.1007/s10195-014-0297-8
21. Anizar-Faizi A, Hisam A, Sudhagar KP, et al. The outcome of surgery for fractures of the acetabulum that are displaced. Malays Orthop J. 2014;8(3):1-6. doi:10.5704/MOJ.1411.001
22. Ferguson TA, Patel R, Bhandari M, et al. Fractures in the acetabulum of patients 60 years or older A radiological and epidemiological study. J Bone Joint Surg Br. 2010;92(2):250-257. doi:10.1302/0301-620X.92B2.22488
23. Giannoudis PV, Da Costa AA, Raman R, et al. Double-crush syndrome after acetabular fractures. It is a sign of poor prognosis. J Bone Joint Surg Br. 2005;87(3):401-407. doi:10.1302/0301-620X.87B3.15253
24. Galvagno SM, Massey M, Bouzat P, et al. Relationship between revision of the trauma score and the severity score and the implications for the prehospital trauma triage. The Prehosp Emergence Care. 2019;23(2):263-270. doi:10.1080/10903127.2018.1489019
25. Hoke Miller MH, Usul E, Ozkan S. Comparison of Trauma Severity Scores (ISS NISS, RTS BIG Score, TRISS) among multiple victims of trauma. J Trauma Nurs. 2021;28(2):100-106. doi:10.1097/JTN.0000000000000567
26. Elkbuli A, Yaras R, Elghoroury A, et al. Comorbidities in the severity of trauma scoring system: improving the the current system of trauma scoring. American Surgery. 2019;85(1):59-63. doi:10.1177/000313481908500130
27. Kuo SCH, Kuo PJ, Chen YC, et al. The new exponential severity score for injuries with the severity score of injury and the newly developed injury severity score for trauma patients A cross-sectional study. A PLoS one. 2017;12(11):e0187871. doi:10.1371/journal.pone.0187871
28. Cornwall R., Radomisli T. Nerve injury after an injury to the hip that causes traumatic dislocation. Clin Orthop Relat Res. 2000;377(377):84-91. doi:10.1097/00003086-200008000-00012
29. Dunbar RP, Gardner MJ, Cunningham B, et al. Sciatic nerve impingement in two-column acetabular fractures: report of two cases and a an analysis of literature. J Orthop Trauma. 2009;23(1):80-83. doi:10.1097/BOT.0b013e318190cfa0
30. Dikici F, Kale A, Ugras AA, et al. Sciatic nerve localization in relation to the location of the Hip anatomical study. Hip Int. 2011;21(2):187-191. doi:10.5301/hip.2011.6491



Understanding Leg Pain: Causes, Symptoms, and How Chiropractic Care Can Help

Are Core Strengthening Exercises Effective for Lower Back Pain Relief?

Nerve Root Compression: Understanding, Symptoms, and Effective Treatments

Understanding and Treating a Herniated Disc: Your Guide to Relief and Recovery

Lower Back Pain: What’s Really Going On and How You Can Feel Better

Understanding Sciatica and Radiculopathy: Causes, Symptoms, and Management

How Often Should You Exercise to Maintain Lower Back Health?

What Are the Top 10 Exercises for Sciatica Pain Relief?

How Does Proper Hydration Reduce Muscle Pain Naturally?

Are Mesh Back Chairs Better for Sciatica Pain Relief?

How Does Stretching Help in Easing Sciatica Discomfort?

What Are the Top 10 Herbal Remedies for Natural Muscle Pain Relief?

How Does Regular Exercise Help Alleviate Lower Back Pain?

How Does Aging Contribute to Chronic Lower Back Pain?
¿Desaparecerá el entumecimiento de los pies con ciática?

How Does Heat Therapy Provide Natural Relief From Muscle Pain?

How Effective Are Herbal Supplements for Alleviating Sciatica Pain?
The Pain Tape Game: Does KT Tape Help With Sciatica?

Will Foot Numbness with Sciatica Go Away?

What Causes Sciatica Nerve Pain
How To Get Sciatica To Stop Hurting
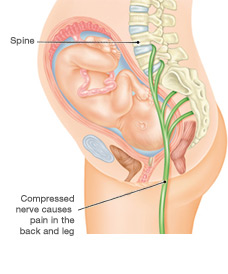
How To Get Rid Of Sciatica Pain During Pregnancy
How To Drive With Sciatica

Will Sciatica Show Up On MRI
How To Fix Sciatica Pain Fast
How To Help Sciatica Pain Naturally
How To Help Sciatica Pain At Home
How To Know Its Sciatica Pain