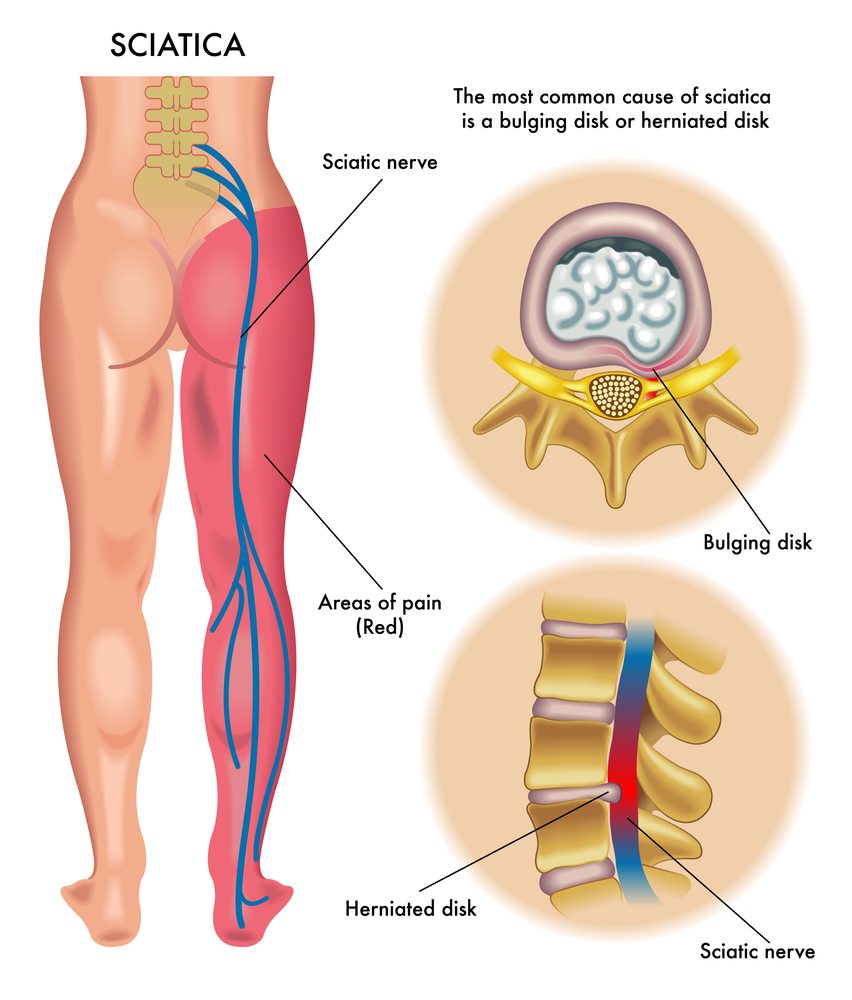
Sciatica
Anatomical features of sciatic and femoral nerves TCRM — Dove Medical Press

Introduction
The total hip joint arthritis (THA) is a successful and proven treatment for patients suffering from Crowe kind-IV hip developmental dysplasia (DDH). However, the risk of postoperative nerve injuries in Crowe type IV patients, which ranged between 7.35 percent up to 10 percent, is considerably more than in other patients with an average of 0.08%-3.7%.1-3 Injuries to nerves after THA is a devastating negative complication that severely impacts the postoperative recovery, functional training as well as the quality of life.4 Limb lengthening as well as inadequate soft-tissue conformity were regarded as risk factors for injuries to the nerves during hip replacements to Crowe Type-IV DDH patients.5-7 Yet, Eggli8 and other researchers9,10 discovered that nerve damage was the most likely to be caused by mechanical direct or indirect injury, not caused through limb lengthening by on its own.
THA in adult patients suffering from Crowe type IV DDH is a difficult technical procedure that is technically difficult. Due to the femoral up dislocation and the abnormal pelvic anatomy The course of the sciatic and femoral nerves can change in line with the dislocation. Therefore, the complex procedure can be associated with greater chance of sustaining direct or indirect nerve injury. An understanding of the path and anatomical properties of sciatic and femoral nerves of patients suffering from Crowe type-IV DDH can help to reduce the chance of injury to the mechanical nerve in the aftermath of THA. 11-14 But, the specifics of peripheral nerve pathway of the hip that is dysplastic has not been thoroughly studied. 15 This study will investigate the anatomical and course of the sciatic and femoral nerves for unilateral Crowe type IV DDH patients who undergo the computed tomography (CT).
Patients and Methods
Patients suffering from unilateral Crowe type-IV DDH were enrolled retrospectively in our center from February 2018 until February 2020. Criteria for inclusion: 1. A hip has Crowe type-IV DDH , and one hip normal developed, that is it has a central-edge angle higher than 25deg. 16. 2. Female, 3. Age: 18-50 years old, 4. Height: 150-170cm, 5. BMI: 20-30kg/m2. Exclusion criteria: 1. History of infection/surgery/trauma in either hip, 2. Nerves in the peripheral limbs lower than that of the limb, disorders like poliomyelitis sequelae 3. The angle between the femoral longitudinal axis and the pelvic median axis is more than 15 deg on CT localization images 4. The angle between the line of inter-teardrop as well as horizontal lines is more than 10 degrees in CT localization images. Our study protocol was ratified through the Ethics Committee of Chinese PLA General Hospital and informed consent was obtained from study participants prior to commencement of the study.
CT Scan Protocols and Parameters
The CT scan (Brilliance ICT, Philips Healthcare, Netherlands) was completed in supine and covered the pelvis and the proximal the femur. The scanning parameters were defined as follows: layer thickness: 0.625mm, pitch: 5mm, kVp: 120kVp mA: 200mA, and field of vision (FOV) 500mm, resolution of the image is 512×512 matrix.
Measurements
We chose reference transverse sections across a variety of key locations (Figure 1: A: anterior superior iliac spinae, B: the medial region of the acetabular wall’s inner wall, C: the inferior margin of teardrop and D: ischial tuberosity) in the CT soft hip tissue window by using a picture archiving and communication technology (PACS, Knowlesys Software Technology Co., Ltd., China) in our institute. We also identified the the sciatic and femoral nerves in accordance with anatomical adjacency relationships as well as the nerve CT numbers (40-60) (Figure 2.).
|
Figure 1. Transverse sections that show selected important locations (A A: the anterior inferior iliac spine B: acetabular internal wall. C refers to the the inferior border of the teardrop and D: ischial tuberrosity). |
|
Figure 2. Ct scans of the axial plane that show the sections that are used to evaluate for the femoral nerve (indicated by a downward an arrow) as well as the sciatic nerve (indicated by an up an arrow) in the cranio-caudal direction. A1 C1, B1, and D1 were affected hips, while A2 B2, and D2 was healthy. Distances in the form of lines (indicated by a white line) between bony landmarks that are adjacent to each other. ( A) Distance from sciatic nerve’s posterior edge of the iliac crest segment ( B) length of sciatic nerve to the posterior acetabular wall , and distance from the femoral nerve towards the anterior acetabular walls, section ( C) Distance from the sciatic nerve towards ischium as well as distance from the pubis to femoral nerve sections ( D) Distance between sciatic nerve and Femoral nerve to femur. |
After verifying the location of nerves the distance between their linear position to the bone landmarks in the pelvis or femur were determined (Figure 2.). The measurements were performed by two postgraduate students studying orthopedics. They repeated the measurements two weeks after. Screenshots from CT images were taken during the measurement and in the event that the results were different in any way or the location of the nerve was unclear the senior orthopedic surgeon was consulted to make the decision. The average measurements were used to compare the results.
Statistics
Analysis of statistics was conducted using SPSS22.0 (IBM Company NY, USA) and power analysis was done using PASS15.0 (NCSS, LLC. Kaysville, USA). All indices were subjected the normality test. Those that were normal distributions were expressed as mean plus standard deviation. All distances across both sides were evaluated using the pairedand test. test. The intra-class correlation coefficients (ICC) were used to determine the consistency of measurements. ICC values varied between 1 and 0 and the degree of consistency was poor (k=0-0.4) moderate (k=0.4-0.6) or significant (k=0.6-0.8) or nearly complete (k=0.8-1) accordance. The criteria for the presence of a statistically significant distinction was p<0.05.
Results
CT scans of the bilateral hips for 21 women suffering from the unilateral Crowe Type-IV DDH were selected for this investigation (Figure 3.). The patients’ basic information was presented in Table 1. The accuracy of the measurement results was near 100%, with an ICC>0.81. While the comparison power of the distance from the pubis (0.58) and the femur (0.74) was minimal, the strength of comparison of distances from femoral nerve to anterior acetabular walls (1.00) in addition to distances from the sciatic nerve to the posterior wall of the acetabular (1.00) and the femur (0.93) were both convincing.
|
Table 1. Demographic Data |
|
Figure 3. Diagram of the flow of a patient. |
In the section A, the median distance of sciatic nerve to the posterior edge of the iliac crest was 10.89+-0.50mm in healthy hips and 11.03+-0.65mm in the affected hip there was no significant difference between the two hips (p=0.487). It was noted that the femoral nerve is located far away from the area of operation and there was no measurement.
In the section B, the distance between sciatic nerve and anterior acetabular wall in the injured hip (30.70+-6.68mm) was significantly higher (p<0.001) than the distance in normal hip (20.07+-2.08mm) The distance between the femoral nerve and anterior acetabular walls in the damaged hip (13.20+-3.59mm) was significantly lower (p<0.001) than in the healthy hip (16.58+-5.12mm).
In the section C, the distance between sciatic nerve and the ischium was 13.98+-3.24mm in the healthy hip and 13.30+-2.90mm in the affected hip. there was no difference in the bilateral direction (p=0.429) and the distance between the femoral nerve and pubis in the affected hip (26.2+-6.90mm) had been significantly greater (p=0.036) than in the healthy hip (21.70+-2.17mm).
In the section D in section D, the distance from the sciatic nerve to femur of the affected hip (15.62+-1.11mm) was significantly higher (p=0.001) than the distance in the healthy hip (14.52+-0.86mm). The distance from the femoral nerve to femur in the affected hip (30.40+-5.67mm) was significantly higher (p=0.013) than that of normal hip (34.36+-5.33mm). The exact values are given in Tables 2 and 3.
|
Table 2. Distinction from the Sciatic Nerve and Bony Marks for Each Section |
|
Table 3. The Distance From Femoral Nerve and Bony Marks on Every Section |
Discussion
In comparison to healthy hips the femoral nerve of affected hips shifted further away from the femur as it grew closer to the an anterior wall of the acetabular. The distances of the sciatic nerve towards the posterior wall of the acetabular as well as the femur in hips with a problem were more than those of healthy hips.
Understanding the anatomy of the sciatic and femoral nerves within the hip area could reduce the risk of injury to nerves when undergoing THA. 17-19 The previous studies of the peripheral nervous system and its its course were mostly built on the magnetic resonance image (MRI) as well as cadaveric or human specimens. But, CT might be a better option for evaluating the nerve courses in the case of DDH. 20-25 On the other hand, MRI was not a routine test for DDH patients, and it is not able to clearly demonstrate bony landmarks. Furthermore, it could increase the expenses for medical care solely for the purpose of monitoring the course of nerves. However it was difficult to locate cadaveric donors with DDH. Numerous researchers have confirmed that CT is a standard examination prior to surgery in Crowe Type-IV DDH patients, can precisely determine the sciatic nerve and femoral nerve. 21,26,27
At present, there has been just one study that was conducted on the field of nerve pathology in patients suffering from DDH. In the year 2015, Wang et al 15 utilized CT to examine the course of nerves in DDH patients and then summarized the anatomical features of the sciatic nerve. They discovered that sciatic nerve was situated close to the ilium and ischium however, it was a bit far from the hip’s femur as compared to its location on the hip that is healthy for those suffering from bilateral DDH. 15 The findings of the study will assist surgeons to better understand the causes of the development abnormalities in soft tissues within the hip joint of patients suffering from DDH and reduce the risk of injury to the nerve. However, there were some flaws with their study. For one the study didn’t contain Crowe type-IV DDH that was at the greatest risk of injury to nerves. Furthermore, the reference area that was used for all measurements was femur-based as well as the landmarks of the femur varied according to the dislocation’s level, which diminished the possibility of comparing the two nerves’ anatomical positions. Additionally, their measurement zone was not able to include the area above the acetabulum and the region below the lesser trochanter. These were typically the operating regions for Crowe type IV DDH patients. Fourthly just the sciatic nerve however, not the femoral, nerve was studied.
The femoral nerve injury was responsible for 27.78 percent (5/18) of all nerve-related injuries that occurred following operation for Crowe type IV DDH. 5 But, previous research has shown that the femoral nerve was resistant to distraction than the sciatic nerve. Moreover, limb lengthening could not be the sole reason for femoral nerve injuries. 11,12 Our findings provide a new explanation for the femoral nerve injury within Crowe type IV DDH from a nerve course view. The nerve that runs through the femoral region was located 1.3 centimeters of the anterior acetabular ridge, incorrectly positioning the retractor prior to the acetabulum, or prolonged traction can result in injury to the femoral nervous system. Furthermore, an overhanging acetabular sleeve was a typical sacrifice to ensure cup stability during Crowe type IV DDH hip replacement. The femoral artery, which comes from the lumbar plexus, curled through the anterior Acetabulum and into the an femoral triangular. If the femoral nerve was stretched and tensed, with less arc, injury to nerve occurred due to contact with the edge of the anterior portion of the overhanging the acetabular cup, causing.
A few studies have confirmed that the position of the retractor in the acetabulum anterior region is a risky step for nerve injury to the femoral. Shubert et al 26 studied the location of Acetabular retractor and its relationship to the adjacent neurovascular structures CT scanning and also cadavers. They discovered an anterior inferior iliac spina is the most secure place for the anterior acetabular retractor. with an inferior progress through the posterior wall. the distance to the femoral nerve bundle shrinks. 26 In our study the distance between the femoral nerve and the anterior acetabular wall was less when we studied Crowe type-IV DDH in comparison to the normal hips, which could make it more likely for nerve injury to the femoral.
The benefits of this study are evident in the following areas. First of all the study was limited to unilateral Crowe type-IV DDH cases were identified which eliminated the impact of other factors like dimensions of the body on results through an individual-control design. Additionally, demographics like gender and age, height and weight were deemed to be valid in addition to previous medical history and neurological autoimmune disorders were not considered to affect the findings. In the end, it was the bones of the pelvis not the femur that were selected as the reference points which were unaffected by height or the femoral dislocation.
However, this study also has a few issues. The first is that the criteria used were very narrow and excluded almost 70 percent of the people who had Crowe IV DDH cases, which makes the number of cases included in this study rather tiny. The second issue was that the postoperative neurological complications associated with these cases were not examined and it was impossible to determine a correlation between anatomical characteristics and the clinical outcome. Thus, we did not assess the real effect of the abnormalities in nerve circulation on the postoperative neurological functioning. The third reason is that CT tests in the in supine positions do not accurately reveal the state of the brain in the more lateral position. Fourth, the morphological analysis of linear distances in various CT sections may be affected by various factors, including patient height, position of the scanner, the chosen CT section, etc. While we have established strict criteria for inclusion and exclusion to limit their influence however, there is a some degree of error with this technique. Therefore, a more thorough geometrical analysis based on morphometry using 3D reconstruction could yield more intriguing results and will benefit the clinical application more.
Conclusion
Females with the unilateral Crowe type-IV DDH The femoral nerve that is affected in the hip is closer to the an anterior acetabular wall than in a healthy hip.
Data Sharing Statement
The data that were used or analyzed in this study can be obtained from the author of the study upon reasonable requests.
Acknowledgments
The study protocol was approved from the Ethics Committee of Chinese PLA General Hospital and informed consent was received from study participants prior to commencement of the study. All procedures were carried out in accordance with those guidelines in the Declaration of Helsinki. We have received consent to publish the study. Ping Song and Xiangpeng Kong are co-first authors of this study.
Contributions to Authors
The authors all contributed in a significant way to the study published, whether it was in the design, conception of the study, design, implementation and acquisition of data the analysis or interpretation of data, or any of the above areas. They took part in drafting, revising , or critically reviewing the article approved the final version to be published. are in agreement with the journal to which the article was submitted and agreed to be accountable for every aspect associated with the research.
Finance
This study was financed by 1. Beijing Municipal Natural Science Foundation (M22016), 2. Clinical Application-oriented Medical Innovation Foundation from National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation and Jiangsu China-Israel Industrial Technical Research Institute Foundation (2021-NCRC-CXJJ-ZH-01), 3. 3. National Natural Science Foundation of China (81772320).
Disclosure
The authors do not report any conflicts of interest in the study.
References
1. Farrell C.M, Springer BD, Haidukewych GJ, Morrey BF. Motor nerve palsy in the wake of primary hip arthroplasty. J Bone Joint Surg Am. 2005;87:2619-2625.
2. Fleischman A.N., Rothman RH, Parvizi J. Femoral Nerve-Pasty Following Total Hip Arthroplasty The incidence and the course of Recovery. J Arthroplasty. 2018;33:1194-1199.
3. Wang D, Zeng W-N, Qin Y-Z, Pei F-X, Wang H-Y, Zhou Z-K. Long-Term Effects from Cementless total hip arthroplasty Patients with High Hip Dislocation after childhood pyogenic infection. J Arthroplasty. 2019;34:2420-2426.
4. de Bruijn IL, Geertzen JHB, Dijkstra PU. Functional outcome after peroneal nerve injury. int J Rehabil Res. 2007;30:333-337.
5. Kong X, Chai W, Chen J, Yan C, Shi L, Wang Y. In-operative monitoring of the sciatic and femoral muscles in hip replacement for development dysplasia that is high-riding. Bone Joint J. 2019;101-B:1438-1446.
6. Nercessian OA, Piccoluga F, Eftekhar NS. Postoperative sciatic and femoral nerve palsy with reference to leg lengthening and medialization/lateralization of the hip joint following total hip arthroplasty. Clin Orthop Relat Res. 1994;1:165-171.
7. DeHart M.M., Riley LH. Injuries to the hip nerves in total arthroplasty. J Am Acad Orthop Surg. 1999;7:101-111.
8. Eggli S, Hankemayer S, Muller ME. Nerve palsy following the lengthening of the leg in total replacement arthroplasty to treat hip dysplasia due to developmental development. J Bone Joint Surg Br. 1999;81:843-845.
9. Lai K-A, Shen W-J, Huang L-W, Chen M-Y. Cement-free total hip arthroplasty and equalization of the length of the limb in patients suffering from unilateral Crowe type IV hip dislocation. J Bone Joint Surg Am. 2005;87:339-345.
10. Weber ER, Daube JR, Coventry MB. Peripheral neuropathies resulting from Total Hip Arthroplasty. J Bone Joint Surg Am. 1976;58:66-69.
11. de Medinaceli L, Leblanc AL, Merle M. The functional consequences of nerve stretching isolated Experimental long-term static load. J Reconstr Microsurg. 1997;13:185-192.
12. Lazansky MG. Complications revisited. Part of the debit that comes with complete hip replacement. Clin Orthop Relat Res. 1973;1:96-103.
13. Fei D, Ma L-P, Yuan H-P, Zhao D-X. Comparative study of femoral nerve block with fascia iliaca block to aid in pain control during total hip arthroplasty. A meta-analysis. The Int. J. Surg. 2017;46:11-13.
14. Hasija R, Kelly JJ, Shah NV, et al. Nerve injuries that are associated with the total hip joint arthroplasty. J Clin Orthop Trauma. 2018;9:81-86.
15. Liu R, Liang J, Wang K, Dang Liu R, Wang K, Dang Bai C. Sciatic nerve course in adult patients suffering from unilateral dysplasia developmental of the hip and its consequences for surgery on the hip. BMC Surg. 2015;15:14.
16. Jessel RH, Zurakowski D, Zilkens C, Burstein D, Gray ML, Kim Y-J. Patient and radiographic factors related to pre-radiographic osteoarthritis hip dysplasia. J Bone Joint Surg Am. 2009;91:1120-1129.
17. Rogers BA, Garbedian S, Kuchinad RA, Backstein D, Safir O, Gross AE. Total hip arthroplasty in adults with hip dysplasia. J Bone Joint Surg Am. 2012;94:1809-1821.
18. Cameron H. Eren Cameron HU, Eren Solomon M. Nerve injury in the prosthetic treatment of the hip dysplastic. Orthopedics. 1998;21:980-981.
19. MacKenzie JR, Kelley SS, Johnston RC. Complete hip replacement for coxarthrosis due to congenital dysplasia, and dislocations of the hip. Long-term results. J Bone Joint Surg Am. 1996;78:55-61.
20. Tagliafico A, Podesta A, Assini A, et al. Imaging with MR Imaging of total hip joint arthroplasty: comparison between sequences for studying the sciatic nerve up to 1.5 1. Magn Reson Imaging. 2010;28:1319-1326.
21. Ergun T, Lakadamyali H. CT and MRI to evaluate extraspinal sciatica. Br J Radiol. 2010;83:791-803.
22. Mehta CR, Constantinidis A, Farhat M, Suthersan M, Graham E, Kanawati A. A distance of femoral neurovascular bundle to the hip joint. An intraoperative method to minimize iatrogenic injuries. J Orthop Surg Res. 2018;13:135.
23. Wang T-I, Chen H -Y Tsai C-H Hsu C-H, Lin T-L. Distances between boney landmarks and nearby nerves: Anatomical variables which influence the position of retractors during total hip replacement. J Orthop Surgery Res. 2016;11:31.
24. Guvencer A, Akyer P, Iyem C, Tetik S, Naderi S. Anatomic considerations and the connection between the piriformis muscles and sciatic nerve. Surg Radiol Anat. 2008;30:467-474.
25. Dikici Fils, Kale A Ugras A, Gayretli O, Gurses IA, Kaya I. Sciatic nerve location in relation to the hip’s location An anatomical study. hip int. 2011;21:187-191.
26. Shubert D, Madoff S, Milillo R, Nandi S. The neurovascular structure is close to acetabular retractors during complete hip replacement. J Arthroplasty. 2015;30:145-148.
27. Selkirk GD, Mclaughlin AC, Mirjalili SA. Reexamining the anatomy of the surface of sciatic nerve within the gluteal area in children by using computed tomography. Clin Anat. 2016;29:211-216.



Understanding Leg Pain: Causes, Symptoms, and How Chiropractic Care Can Help

Are Core Strengthening Exercises Effective for Lower Back Pain Relief?

Nerve Root Compression: Understanding, Symptoms, and Effective Treatments

Understanding and Treating a Herniated Disc: Your Guide to Relief and Recovery

Lower Back Pain: What’s Really Going On and How You Can Feel Better

Understanding Sciatica and Radiculopathy: Causes, Symptoms, and Management

How Often Should You Exercise to Maintain Lower Back Health?

What Are the Top 10 Exercises for Sciatica Pain Relief?

How Does Proper Hydration Reduce Muscle Pain Naturally?

Are Mesh Back Chairs Better for Sciatica Pain Relief?

How Does Stretching Help in Easing Sciatica Discomfort?

What Are the Top 10 Herbal Remedies for Natural Muscle Pain Relief?

How Does Regular Exercise Help Alleviate Lower Back Pain?

How Does Aging Contribute to Chronic Lower Back Pain?
¿Desaparecerá el entumecimiento de los pies con ciática?

How Does Heat Therapy Provide Natural Relief From Muscle Pain?

How Effective Are Herbal Supplements for Alleviating Sciatica Pain?
The Pain Tape Game: Does KT Tape Help With Sciatica?

Will Foot Numbness with Sciatica Go Away?

What Causes Sciatica Nerve Pain
How To Get Sciatica To Stop Hurting
How To Get Rid Of Sciatica Pain During Pregnancy
How To Drive With Sciatica

Will Sciatica Show Up On MRI
How To Fix Sciatica Pain Fast
How To Help Sciatica Pain Naturally
How To Help Sciatica Pain At Home
How To Know Its Sciatica Pain